Lower Blepharoplasty in Beverly HillsEverything You Need to Know
Under-eye bags are one of the most universally recognized signs of facial aging, and one of the most persistently frustrating. They appear regardless of how much sleep a person gets. They resist eye creams, cold compresses, dietary changes, and every non-surgical intervention the skincare industry has produced. They affect men and women, appear in patients in their thirties as often as in their sixties, and have a disproportionate impact on how a face reads at rest, making people appear tired, older, or unwell regardless of how they actually feel.
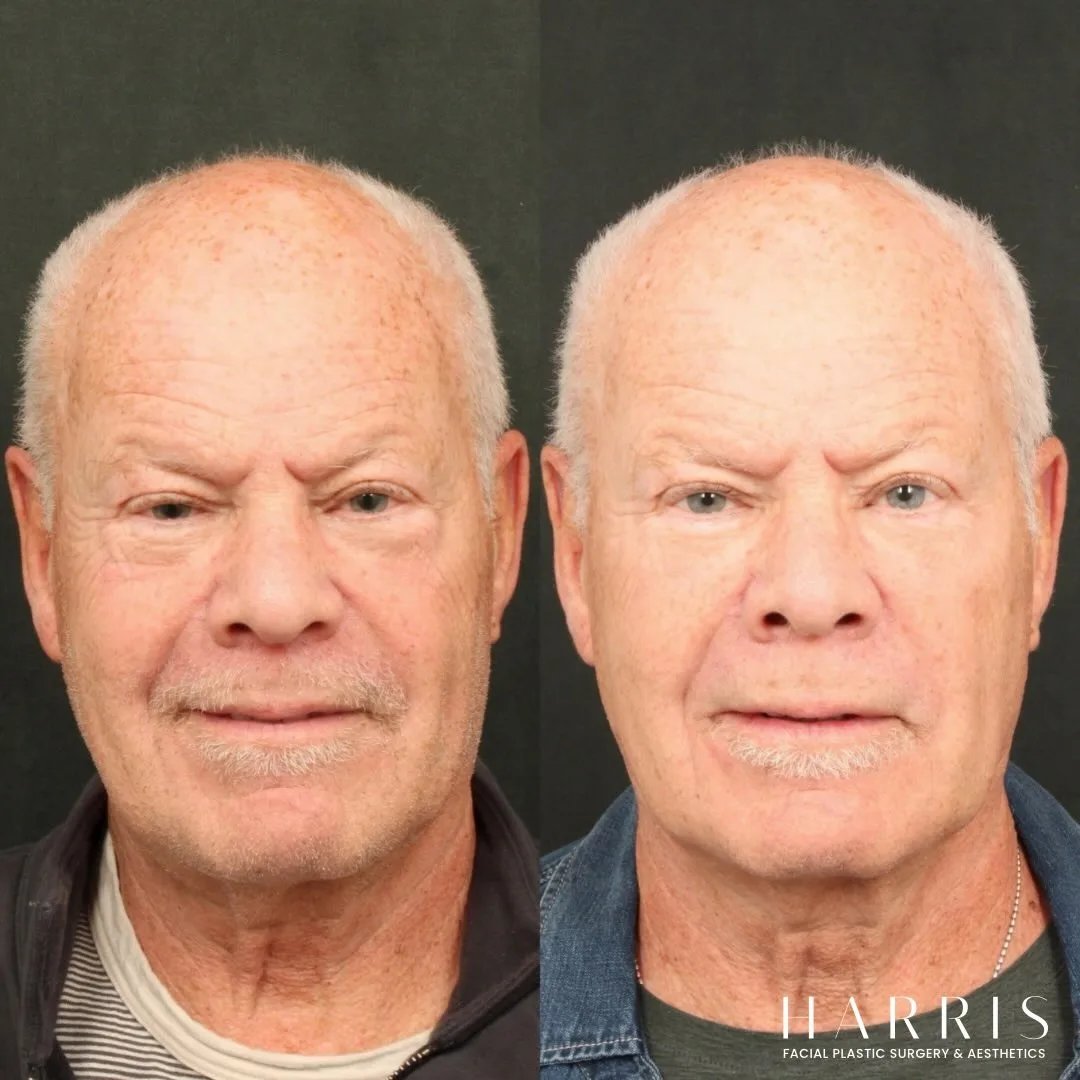
Lower blepharoplasty, eyelid surgery that specifically addresses the lower lid and the under-eye area, is the most effective and permanent solution available for this concern. When performed by an experienced surgeon, the result is a smooth, refreshed lower eye area that looks natural, heals with minimal visible evidence of surgery, and lasts for many years. Dr. William C. Harris at Harris Facial Plastic Surgery & Aesthetics in Beverly Hills performs lower blepharoplasty as one of the core procedures in his facial plastic surgery practice, using a scarless technique for appropriate candidates and a meticulous, anatomy-driven approach across all presentations.
"Flawless facial plastic surgery should never reimagine one's appearance, but revitalize it. — William Harris, MD"
Several other changes contribute to lower eyelid aging alongside fat herniation. The skin of the lower lid loses elasticity and develops crepey texture. The orbicularis oculi muscle, which encircles the eye, can develop a visible roll just below the lash line. The tear trough, the groove at the junction between the lower eyelid and the cheek, becomes more prominent as the cheek descends and the eyelid fat moves forward. And in some patients the lower eyelid itself loses its structural support and begins to droop or sag.
Not all patients present with all of these changes simultaneously, and the treatment plan for lower eyelid rejuvenation needs to reflect what is actually present in each individual. Dr. Harris evaluates the lower eyelid comprehensively at consultation, assessing fat herniation, skin laxity, muscle hypertrophy, tear trough depth, and eyelid position before making any recommendation.
What Lower Blepharoplasty Can Address
Under-Eye Bags from Fat Herniation
The primary indication for lower blepharoplasty is fat herniation causing visible bags. Surgery addresses this by accessing the fat pads through an incision inside the lower eyelid and either removing a conservative amount of the herniated fat, repositioning it into the tear trough area where it fills a deficit rather than creating a bulge, or a combination of both approaches. The result is a lower eyelid that lies flat and smooth against the underlying structure rather than bulging forward.
Excess Lower Eyelid Skin
In patients who have skin laxity in addition to fat herniation, a small amount of skin can be removed through a fine incision placed just below the lash margin. This subciliary approach is used selectively for patients whose skin excess is clinically significant and who have adequate lower eyelid structural support to tolerate the tension of skin removal without the eyelid pulling downward.
The Tear Trough
The tear trough is the grooved depression that runs from the inner corner of the eye diagonally down and out along the eyelid-cheek junction. In many patients, under-eye bags are accompanied by a prominent tear trough that casts a shadow and makes the area look hollow or darkened. Fat repositioning during lower blepharoplasty fills the tear trough from below, smoothing the transition between the eyelid and the cheek without the need for ongoing filler maintenance. For some patients, a small amount of filler or fat transfer complements the surgical result.
Lower Eyelid Skin Texture
The crepey, thin-textured skin that develops on the lower eyelid with age and sun exposure is not directly addressed by blepharoplasty but can be improved with concurrent skin resurfacing. Laser resurfacing or chemical peeling performed at the same time as lower blepharoplasty improves the surface quality of the eyelid skin, producing a result that addresses both the structural change beneath and the surface quality on top.
The Scarless Lower Blepharoplasty: Dr. Harris's Preferred Approach
For patients whose primary concern is fat herniation without significant skin laxity, Dr. Harris uses a transconjunctival approach, in which the incision is placed entirely inside the lower eyelid on the conjunctival surface. This incision is invisible from outside the eye at all times, including during and after healing. There is no external scar from this technique at any stage of the recovery.
The transconjunctival incision provides direct access to the orbital fat compartments of the lower eyelid. Through this access point, Dr. Harris addresses the fat with precision, either removing the appropriate amount from the area of excess or repositioning it into the tear trough depending on what the anatomy requires. The incision is closed with absorbable sutures that do not need to be removed.
The absence of an external scar is not merely a cosmetic advantage. It also eliminates the risk of scar-related eyelid position changes that can sometimes occur with subciliary incisions in patients with less eyelid structural support. For appropriate candidates, the transconjunctival approach is the safest and most efficient route to the underlying structures.
When a Subciliary Incision Is Used
The subciliary approach, in which a fine incision is made just below the lash line, is used when skin removal is necessary in addition to fat management. This occurs in patients who have enough lower eyelid skin excess that the skin will not retract adequately after fat removal and will instead create a baggy appearance even after the underlying cause has been corrected.
The subciliary incision is placed within the natural shadow of the lash line and heals with minimal visible scarring in most patients. The scar matures over three to six months and is typically not detectable at normal social viewing distances when properly placed and closed.
The subciliary approach requires more careful patient selection than the transconjunctival approach because removing skin from the lower eyelid creates tension that can, in patients with inadequate eyelid support, pull the lower lid away from the eye. Dr. Harris performs a snap test and other assessments of lower eyelid tone at consultation to confirm that the eyelid can tolerate skin removal safely.
Fat Removal Versus Fat Repositioning: A Critical Distinction
The decision between removing orbital fat and repositioning it is one of the most consequential choices in lower blepharoplasty planning and one that reflects the evolution of the procedure over the past two decades.
Earlier approaches to lower blepharoplasty routinely removed significant amounts of orbital fat from the lower eyelid to eliminate the bulge. This produced immediate improvement in the bags but frequently created a new problem: a hollowed, skeletonized lower eyelid that looked operated on and aged more rapidly than a naturally full lower lid. Patients who had aggressive fat removal in their forties and fifties often develop a sunken, tired appearance in their sixties that is more difficult to manage than the original bags.
Modern lower blepharoplasty technique, as practiced by Dr. Harris, approaches fat conservatively and preferentially repositions it rather than removing it. Fat repositioning takes the herniated fat from the area where it is creating a bulge and moves it into the tear trough, where it fills a hollow that contributes its own shadow and aged appearance. The result is a double correction: the bulge is reduced and the hollow is filled simultaneously, producing a smooth, youthful eyelid-to-cheek transition that maintains volume and does not hollow with time.
Not every patient is a candidate for repositioning. The decision depends on the degree of fat herniation, the depth of the tear trough, and the structural support of the eyelid. Dr. Harris discusses the approach appropriate for each patient based on a thorough assessment at consultation.
The Procedure: What Happens on the Day of Surgery
Anesthesia
Lower blepharoplasty at Harris Facial Plastic Surgery & Aesthetics is typically performed under local anesthesia with oral sedation. Patients are awake and comfortable throughout the procedure. The eyelid area is thoroughly numbed before any incision is made, and patients generally experience pressure and mild sensation rather than pain during the procedure. For patients who are anxious about being awake during facial surgery, the oral sedation component provides a relaxed, calm state throughout.
The Procedure Itself
Once anesthesia is established, the incision is made according to the planned approach. Through the transconjunctival incision, the orbital septum is opened and the fat compartments of the lower eyelid are accessed. The fat is addressed according to the plan developed at consultation, either through conservative excision, repositioning into the tear trough, or a combination. The incision is closed with absorbable sutures.
When a subciliary approach is used, the incision is made below the lash line and the skin and muscle are elevated to access the underlying fat. After fat management, the skin is gently redraped and any excess is trimmed conservatively before the incision is closed with fine sutures.
The full procedure typically takes forty-five minutes to one and a half hours depending on the complexity of the case and whether it is being performed bilaterally or in combination with upper blepharoplasty.
Recovery After Lower Blepharoplasty
The First Week
Swelling and bruising around the lower eyelids are expected in the first week. The degree varies between patients, with some experiencing only mild discoloration and others having more extensive bruising that extends into the upper cheek area. Cold compresses applied for ten to fifteen minutes at a time with breaks between applications are effective for managing both swelling and discomfort in the first forty-eight hours. Head elevation during sleep reduces overnight fluid accumulation.
Patients who had a transconjunctival procedure have no external wound to manage and do not need suture removal. Patients who had a subciliary approach have fine surface sutures that are removed at seven to ten days.
Week Two and Return to Normal Activity
By the end of the second week, most patients are comfortable returning to professional and social settings. Bruising has typically resolved or faded to a level manageable with makeup by day ten to fourteen. Swelling continues to improve over the following weeks. Most patients are surprised by how quickly their social recovery occurs relative to their expectations before surgery.
The Settling Period
Lower eyelid swelling can persist in subtle form for four to six weeks after surgery. During this period the lower lid may appear slightly fuller or less defined than the final result will reflect. The complete settled outcome of lower blepharoplasty is typically visible at three to four months, when all residual swelling has resolved and the tissues have fully integrated with the new fat arrangement beneath.
Combining Lower Blepharoplasty with Other Procedures
Lower blepharoplasty is frequently performed alongside other procedures to produce a more comprehensive periocular or facial rejuvenation result. The most common combinations include the following.
Upper and Lower Blepharoplasty Together
Performing both upper and lower eyelid surgery in the same session, referred to as four-eyelid blepharoplasty or bilateral blepharoplasty, addresses the full periocular area comprehensively and produces a cohesive improvement in the eyes as a whole. Patients who have concerns in both areas benefit from the efficiency of a single procedure, single anesthesia, and single recovery rather than two separate interventions.
Lower Blepharoplasty with Facelift or Midface Lift
The lower eyelid and the cheek are anatomically connected. Descent of the midface contributes to lower eyelid aging by pulling the cheek tissue downward and deepening the tear trough. Combining lower blepharoplasty with a facelift or midface lift that repositions the descended cheek tissue addresses both levels of the problem and produces a more complete rejuvenation of the lower face than either procedure accomplishes alone.
Lower Blepharoplasty with Skin Resurfacing
The crepey skin texture of the lower eyelid is a surface issue that surgical fat management does not directly address. Concurrent laser resurfacing or chemical peeling improves the surface quality of the lower eyelid skin, tightening fine lines and improving tone. This combination produces a result that is more comprehensive than blepharoplasty alone for patients with significant surface aging alongside their structural concerns.
What Results Look Like and How Long They Last
A well-executed lower blepharoplasty produces a lower eye area that is smooth, flat, and appropriately volumized. The under-eye bags are gone. The transition from the eyelid to the cheek is smooth rather than abrupt. The shadow created by the tear trough is reduced or eliminated. The overall expression the eyes project is refreshed rather than fatigued.
The fat that has been removed during the procedure does not return. The positional correction of fat repositioning is permanent. The results of lower blepharoplasty are therefore genuinely long-lasting, with most patients maintaining a meaningful improvement for ten or more years. The surrounding tissue continues to age normally, but the specific structural correction made during the procedure persists.
Patients who protect their skin from sun exposure, maintain consistent skincare habits, and maintain a stable weight tend to see the longest-lasting results. Non-surgical maintenance treatments in the years after blepharoplasty, including skin tightening technologies and periodic filler if volume loss develops elsewhere in the midface, complement the surgical result and extend its longevity.
Choosing the Right Surgeon for Lower Blepharoplasty in Beverly Hills
Lower blepharoplasty is technically demanding surgery. The lower eyelid is a thin, structurally complex area in which small errors in judgment, whether in how much fat is removed, how much tension is placed on the skin, or how the incision is placed, can produce outcomes that are difficult and expensive to correct. The concentration of experienced, fellowship-trained facial plastic surgeons in Beverly Hills makes it an environment where patients have access to a high standard of care, but the differences between providers remain meaningful.
Dr. Harris is an AAFPRS fellowship-trained, double board-certified facial plastic and reconstructive surgeon who completed one of just fifty AAFPRS fellowship positions awarded nationally each year. His training in Palo Alto included mentorship from world-class surgeons and teaching responsibilities at Stanford University. His background as a fine arts student alongside his medical training has given him an eye for proportion and the relationship between facial structures that directly informs how he approaches the aesthetics of every blepharoplasty he performs.

His practice holds a 5.0 rating from more than 101 patient reviews. His patients describe results that look natural and appropriate for their faces, recoveries that were more manageable than expected, and a consultation experience that was thorough, honest, and individualized. To schedule a lower blepharoplasty consultation at Harris Facial Plastic Surgery & Aesthetics, visit harrisfacialplasticsurgery.com or call (310) 880-2117. The practice is located at 301 N. Canon Drive, Suite 208, Beverly Hills, CA 90210.
Common Questions
Frequently Asked Questions
Lower blepharoplasty is a surgical procedure that addresses the lower eyelid area, including under-eye bags caused by herniated orbital fat, excess skin laxity, and crepey or loose lower eyelid skin. The procedure can be performed through an incision inside the lower eyelid, leaving no external scar, or through a fine incision just below the lash line when skin removal is also required. The result is a smoother, less puffy, more rested lower eye area.
Transconjunctival blepharoplasty places the incision inside the lower eyelid, completely hidden from external view. It is ideal for patients whose primary concern is fat herniation without significant skin excess. The subciliary approach places a fine incision just below the lash line and is used when skin removal or tightening is also required. Dr. Harris evaluates each patient's anatomy at consultation to determine which approach is appropriate.
Yes. Lower blepharoplasty that addresses the herniated orbital fat causing under-eye bags produces a permanent correction of those bags. The fat that is removed or repositioned does not return. The surrounding tissues will continue to age normally over time, but the specific bags that were present before the procedure are permanently corrected.
Lower blepharoplasty at Harris Facial Plastic Surgery is typically performed under local anesthesia with oral sedation, meaning the patient is awake but comfortable and the eyelid area is fully numbed. General anesthesia is not required for most cases. When lower blepharoplasty is combined with a facelift or other more extensive procedure, the anesthesia approach is adjusted accordingly.
Recovery from lower blepharoplasty is similar to upper blepharoplasty. Bruising and swelling are most pronounced in the first week and resolve progressively over two weeks. Most patients are comfortable returning to professional and social settings at ten to fourteen days. Swelling in the lower eyelid area can persist in subtle form for several weeks beyond this, but is typically not visible to others.
Yes. Fat repositioning, in which the herniated orbital fat is moved from the area of excess to the area of the tear trough where volume is deficient, is an advanced technique that addresses both the under-eye bag and the hollowness below it simultaneously. It avoids over-removal of fat and produces a smooth transition between the lower eyelid and the cheek. Dr. Harris determines the appropriate fat management approach based on each patient's anatomy.
The tear trough is the groove or depression that runs from the inner corner of the eye diagonally down and outward along the junction between the lower eyelid and the cheek. In many patients, under-eye bags are accompanied by a prominent tear trough that makes the transition between the eyelid and cheek look hollow or shadowed. Fat repositioning during lower blepharoplasty can fill the tear trough from below, producing a smooth eyelid-to-cheek contour without the need for filler.
Yes, and it frequently is. Lower blepharoplasty is commonly combined with upper blepharoplasty for comprehensive periocular rejuvenation, with a facelift or midface lift, with fat transfer to the cheeks, or with skin resurfacing treatments that improve the surface texture of the lower eyelid skin. Dr. Harris discusses combination options at consultation based on each patient's full facial picture.
Lower blepharoplasty carries the standard risks of any surgical procedure including infection, bleeding, and anesthesia reaction, as well as eyelid-specific risks including dry eye, temporary or persistent eyelid position changes, asymmetry, and in rare cases ectropion, a condition in which the lower eyelid turns outward. Choosing a fellowship-trained, board-certified facial plastic surgeon with specific experience in eyelid surgery significantly reduces the risk of these complications.
Consultations can be scheduled at Harris Facial Plastic Surgery & Aesthetics, located at 301 N. Canon Drive, Suite 208, Beverly Hills, CA 90210. To book, visit harrisfacialplasticsurgery.com or call (310) 880-2117. Dr. Harris evaluates each patient's lower eyelid anatomy in detail at consultation and develops a personalized surgical plan with complete information about technique, recovery, and cost.

Dr. William C. Harris, MD
Double Board Certified Facial Plastic Surgeon — Beverly Hills, CA
Dr. Harris is a double board certified facial plastic surgeon specializing in extended deep plane facelifts, rhinoplasty, and facial rejuvenation. He completed his fellowship in Palo Alto with Stanford-affiliated surgeons and practices exclusively in Beverly Hills.
About Dr. Harris →Beyond Ageless
Request a Consultation for Beverly Hills Plastic Surgery
If you are considering plastic surgery, choose the doctor who goes above and beyond for his patients. Dr. William Harris makes it his mission to deliver artful, innovative, and detailed surgical and non-surgical procedures to help you live more beautifully every day. Schedule a consultation today to start your journey.
Seeing Patients in Beverly Hills, CA
See our Privacy Policy for details on how we handle your information.
Monday - Friday: 9am - 5pm
Saturday: 9am - 12pm

© 2026 Harris Facial Plastic Surgery & Aesthetics
All Rights Reserved | Sitemap | Privacy Policy | Patient Payment Database | Accessibility